
The “Transitions of Care” zoom meeting’s goal is to improve communication between case management and community providers, especially related to readmissions and start of care following a hospital visit. The meeting is facilitated by Amy Schmidt, however, this meeting has contributions from multiple case managers from several Oregon and Washington hospitals. It is an open invitation for any case manager to join the discussion. Some may join only once, some participate in only specific topics, a few routinely listen but only participate by chat box, – any/all levels of participation are welcome. Initially the calls were geographically specific, but we found that many issues overlapped regardless of region. Now, all Oregon & Washington providers meet together on the 1st Tuesday of EVEN months at 11:30am. This ZOOM call provides thirty minutes of engagement with hospital case management staff, followed by 15 minutes of provider discussion if needed. Any case manager or provider can send agenda topics to Amy Schmidt.
Next meeting: April 7, 11:30am
Zoom Meeting link:
https://us02web.zoom.us/j/
Meeting ID: 503 505 5865
One tap mobile
+16694449171,,5035055865# US
Resources from past meetings:
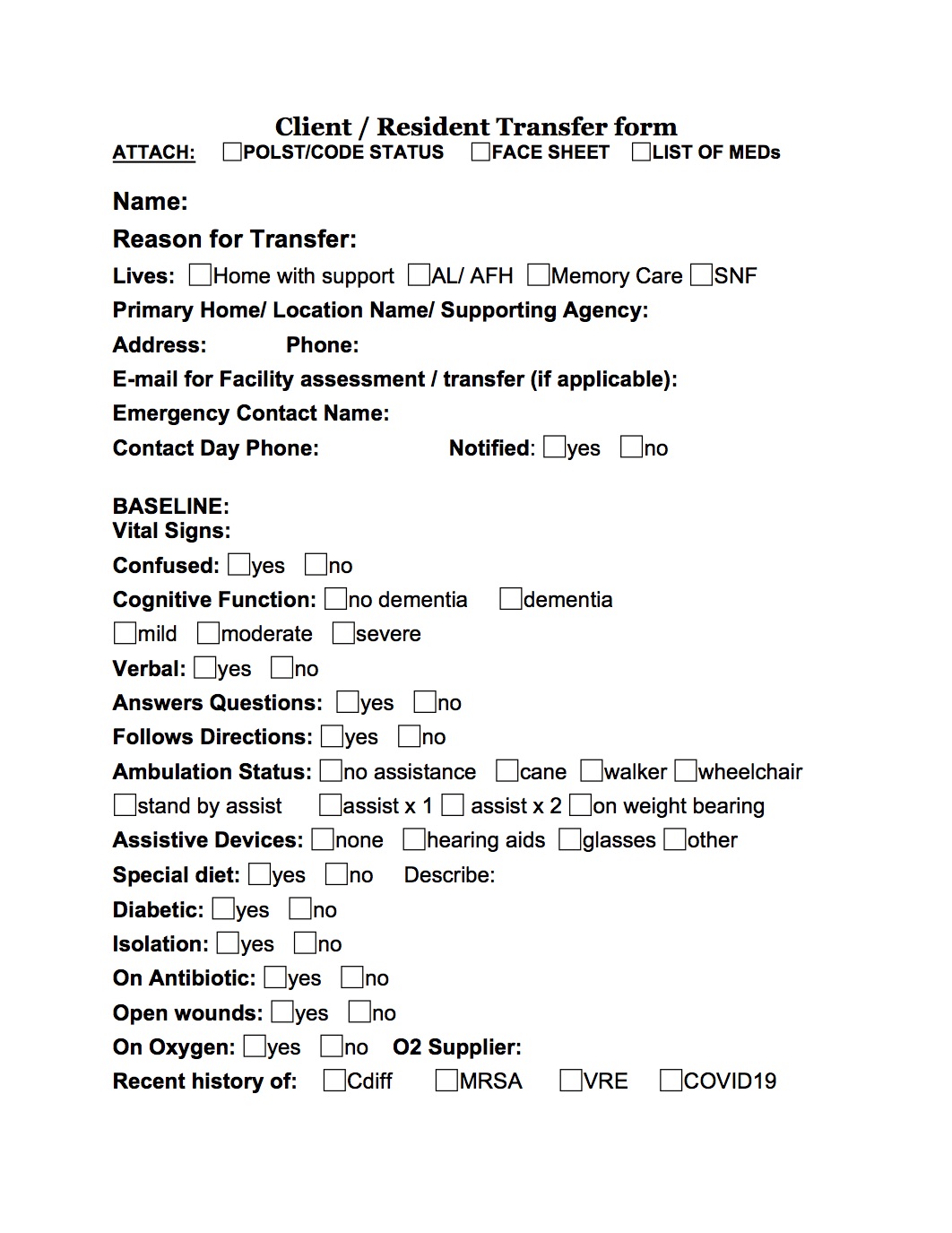
View Client/Resident Transfer Form
Download Client/Resident Transfer Form
{kind=link}
Link to slides_Working with Clinic Case Managers for Physician Case Management- Jenelle (December 2025 meeting)
- Link to the June 4th Zoom Chat: Chat from the Transitions of Care zoom call June 4th
-
Links for families to OPT out of having their information shared and sold:
- Here is the link to the Long Term Care Referral Agency site, where you can see every registered agency and the rules governing them: https://ltcr.oregon.gov/FAQ#RP1
- Link to the latest OAR from September 2022 about LTCRS: 2022-09-15 Perm 411-058
- Link to OSRAA meetings (Oregon Senior Referral Agency Association), Non-members can RSVP for and attend our quarterly meetings: https://osraa.com/rsvp-meeting/
- Link to OSRAA Bylaws: OSRAA By-laws 2023 review-2
- Link to OSRAA Code of ethics: OSRAA-Code-of-Ethics-Preamble-and-Articles-2021
- Link to ASRP (Association of Referral Professionals of Washington): https://www.asrpwa.org/contact-us/
Save the dates, Every 2 months on the First Tuesday.